| Journal of the POMA - Vol 70, No 2 - June 2026 |
From the Editorial Board
Serpent, Selah, and Mario
By Samuel Garloff, DO, PCOM '78
WGRP here. The serpent in the title does not reference the serpent of Genesis, the serpent contained at a roadside attraction, or the serpent found in a reptile house at a zoological garden. The serpent in the title represents a musical instrument from the time of the Renaissance. It’s a curious thing, made of wood, covered in leather, coiled in serpentine fashion. An early wind instrument, it featured a large metal mouthpiece and therefore is now referred to as a brass instrument. Historians claim it to be a precursor of the modern-day tuba. Often, however, its musical contribution to the orchestra is rewritten for contrabassoon.
Selah is a fascinating word that appears 71 times in Psalms. It has never truly been translated from Hebrew to English. It is now thought to represent pause, or reflect, or indicate the initiation or cessation of music. Its use in Psalms could certainly fit any of the preceding.
Mario Lanni (1936-2026) served as this association’s Executive Director for decades. I have chosen not to add his honorary doctorates after his name as I never heard him use them publicly. It simply wasn’t his style. Once, in a private conversation, I brought the subject up; he responded to my query quickly and quietly. He was genuinely proud to have received honorary doctorates from both PCOM and LECOM, but he was not boastful. We never again spoke of the matter.
Mario was my friend. Our relationship started oddly. Shortly after I became president of POMA, he asked if I would sign a letter to the AOA in support of one of the schools. I refused, stating my belief that the association was for physicians and supported physicians, not related entities. I told him the immediate past president or president-elect could sign, but I would not. The issue was never brought up again.
After my year as president was over, Ellen and I invited Mario and Deborah to dinner at a restaurant in Harrisburg. It was a pleasant evening. Soon afterward, the four of us started going out once a month to diners, dives, and occasionally something more upscale. We looked forward to our time together.
|
Angela D. Zawisza, DO, FAAP, Installed as 115th POMA President
Angela D. Zawisza, DO, FAAP, was installed as POMA’s 2026–2027 President during the Presidential Installation Banquet at POMA’s Annual Clinical Assembly on May 15, 2026, at Kalahari Resorts & Conventions in Pocono Manor, Pennsylvania.
Dr. Zawisza has been a member of the association since 2007. She began her leadership service within the association as a District Trustee in 2020. She was elected Vice President in 2024 and President-Elect in 2025. She continues to serve as a delegate to both the POMA House of Delegates and the American Osteopathic Association House of Delegates.
Dr. Zawisza is chair of the Department of Pediatrics at Lehigh Valley Hospital–Schuylkill in Pottsville, Pennsylvania. Board-certified in pediatrics, she graduated from Illinois Wesleyan University in Bloomington, Illinois, and earned her medical degree from Des Moines University College of Osteopathic Medicine in 2007. She completed an internship and pediatric residency at Geisinger Medical Center’s Janet Weis Children’s Hospital in Danville, Pennsylvania.
|
In addition to serving as POMA’s President for 2026–2027, Dr. Zawisza serves as the champion of POMA’s Communications Pillar and as a member of the POMA Foundation Board of Directors. A Fellow of the American Academy of Pediatrics, she is also a member of the American Osteopathic Association.
The following is a transcript of Dr. Zawisza’s speech delivered during the Presidential Installation Banquet:
|
Can't See, Can't Hear, Can't Afford Viagra
By Samuel Garloff, DO, PCOM '78
Well, I can afford Viagra, but with the nitrates I take, it would be as sensible as adding C-4 to a completed IED. Every morning, I wake up searching for my eyeglasses and hearing aids. Then after my established morning ritual, I settle down to a mug of coffee to kick-start my chest pump. Mug number 2 is for swallowing my morning meds…all 13 of them. Remember learning that more than five meds is potentially dangerous due to the possibility of reduced efficacy and possible interactions? I get yearly thank-you cards from the sons and daughters of pharmacists acknowledging my part in paying for their university education.
It doesn’t stop there. An hour or two later I consume 3 additional meds with my morning bagel or oatmeal. This ritual is repeated with my evening meal. Nighttime signals the consumption of an additional 8. This brings the daily total to 13+3+3+8=27. That, of course, is if I don’t use any Nitro sl prn.
When I take off my shirt, my chest and abdomen demonstrate the sequelae of long-forgotten surgical interventions. Not to brag, but Rand-McNally has purchased my integument to study and learn how to add red lines to their atlas maps after my demise.
|
A Sunken Spirit
By Melissa P. Broyles, DO, PCOM '97
A panicked voice cries out from bed A: “I need a doctor. I need a doctor. My body is shrinking.” There lies an eighty-eight-year-old, cachectic woman, fully dressed, with her head at the foot of the bed, staring at the ceiling framed by four blank walls. She pleads with me to examine her, hastily removing her red turtleneck sweater as I draw the dividing curtain. I quickly realize this is Ms. Mosley - the same woman who has been refusing to take her sertraline. After examining her, I clear the clutter from the bedside chair, her only companion.
Ms. Mosley understood her illness well. She had chosen not to pursue aggressive treatment for her cancer and had been on hospice-level care for the past six months. As I sit beside her, I ask the quintessential question: “How would you like to spend whatever time you have left on this earth?” Her sunken eyes meet mine, and after a long pause, she replies softly, “No one has ever asked me that question before.” Then, with conviction, she quickly declares, “I want to glorify God!”
|
Beyond the Exam Room: An Osteopathic Commitment to Patient Rights
By Sindy Paola Hernandez, PCOM OMS-III
For every medical student and future physician, there will come a day when an undocumented patient walks into their office. We are trained not only to treat illnesses but to advocate for our patients and the communities we serve. Advocacy does not end at ensuring medical equity—it extends into every aspect of our patients' lives.
In the words of Dr. Andrew Taylor Still, “The body is a unit; the person is a unit of body, mind, and spirit.”
Health is not just about medical treatment; it is shaped by environment, access to resources, and legal protections. Ensuring that individuals know their rights aligns with the osteopathic belief that a person’s well-being is interconnected with their circumstances.
|
Trends and Outcomes in Residency Matches: Assessing the Post-Merger Landscape for DO and MD Graduates
By Haley S. Jerman, M.S., PA-C, OMS II, Katlyn E. Yebernetsky, M.S., PA-C, OMS II, Shaun-Marie T. Wilson, M.P.H., PA-C, OMS II, Sarah Rosmarin, M.S., PA-C, OMS II, and Christopher B. Divito, Ph.D.
All authors are affiliated with the College of Medicine at Lake Erie College of Osteopathic Medicine at Seton Hill, Greensburg, PA.
Abstract
Context: The effects of the American Osteopathic Association (AOA) and Accreditation Council for Graduate Medical Education (ACGME) merger on match rates for osteopathic (DO) graduates have yet to be fully elucidated. The goal of the merger was to increase equity between DO and allopathic (MD) graduates. Subsequent to the merger, concerns remain regarding parity among DO and MD graduates.
Objectives: To examine trends in residency placements, we analyzed pre- and post-merger match rates for dermatology, neurological surgery, orthopedic surgery, radiology, anesthesiology, and obstetrics-gynecology (OB/GYN) residencies for both DO and MD graduates.
Methods: Data were compiled from the National Resident Matching Program (NRMP) from 2014-2024 and the National Matching Service (NMS) for 2014 - 2019. Additionally, yearly totals of osteopathic and allopathic graduates from the American Association of Colleges of Osteopathic Medicine (AACOM) and the Association of American Medical Colleges (AAMC) were collected. All data were analyzed by linear regression analysis, Spearman’s correlation, and Mann-Whitney U tests using Prism v10.
|
Adrenaline Rush: A Ruptured Pheochromocytoma Masquerading as Abdominal Pain
By Michelle Joyner, DO, MS, Jefferson Northeast, Departments of Internal and Emergency Medicine, Philadelphia, PA; Jacob Dewey, MS4, Philadelphia College of Osteopathic Medicine, Philadelphia, PA; John Keilty, MD, Jefferson Northeast, Departments of Internal and Emergency Medicine, Philadelphia, PA; Zachary Weisner, DO, MS, Jefferson Northeast, Departments of Internal and Emergency Medicine, Philadelphia, PA; Kevin Rolnick, MD, Mayo Clinic Health System, La Crosse, WI
Abstract
Spontaneous retroperitoneal hemorrhage (SRH) from a ruptured pheochromocytoma is a rare, life-threatening condition. We report a 45-year-old man presenting with abdominal pain and hypertension with imaging showing active bleeding near the adrenal gland. Emergency embolization was performed, and blood work confirmed elevated catecholamines. This case demonstrates the importance of understanding the signs, symptoms, pathophysiology, and management of SRH due to suspected pheochromocytoma rupture.
Introduction
Spontaneous retroperitoneal hemorrhage (SRH) is an uncommon and life-threatening condition that may present in any population, though is associated with advanced age and anticoagulation.1 A rare etiology of SRH is from a pheochromocytoma, which is a catecholamine-producing tumor derived from chromaffin cells of the adrenal medulla. Rupture can rapidly produce a catecholamine-induced sympathetic response in addition to hemorrhagic shock due to rapid bleeding in the retroperitoneal space.2 While SRH via a ruptured pheochromocytoma is extremely rare, with only around 65 cases reported, it has a reported mortality rate of 28%.3 SRH can present with a wide variety of symptoms, ranging from abdominal pain, to back or hip pain, and the patient may have hypertension or hypotension, making the diagnosis challenging.1 Our case underscores the unique pathophysiology and management of suspected pheochromocytoma rupture leading to SRH.
|
Enhancing Patient Adherence in the All-Too-Brief Office Visit
By M. Robin DiMatteo, Ph.D.
Distinguished Professor Emerita, University of California, Riverside
Visits to follow up on medication and chronic disease management can be as short as
12 to 15 minutes. What are the most effective strategies that you and your healthcare team can employ to help your patients when you are “ruled by the clock”?
We like to think of the process of medical care as a fairly linear event in which the doctor gives an order and the patient quietly obeys. But what really happens is usually “messier” than that. Most clinicians would probably agree that the clinician-patient encounter can be quite complex, and what the patient does after it can be influenced by a host of unexpected factors.
Decades before they had mountains of data supporting their intuition, many clinicians felt that the hardest part of practicing medicine often wasn't the diagnosis but rather it was the follow-through. It is said that human behavior is the “wildcard” in medical care delivery, and patient nonadherence is a huge and often unmet challenge.
|
Doc's Girls: Sex Workers, a play by Gilbert Kasirsky, DO, Ph.D.
By Samuel Garloff, DO, PCOM '78
This is an original play by the author of Vasectomy, Manhood and Sex, published by Springer Publishing Company. The author describes his new book as “mostly a memoir,” with the events taking place more than a decade ago.
The main character, Dr. Gil Gilstein, is a successful family physician with a military background. He becomes involved in the examination of working girls upon the request of an old friend. Shortly afterward, he becomes more deeply involved with the underworld and discovers his employers traffic not only in the sex trade but in the manufacture, distribution, and selling of narcotics. What his employers don’t realize is that he has been contacted by FBI and DEA agents and has become a government informant.
|
The Healer
By Jacqueline M. Fignar, DO
Devoted doctor
Answers the call of the ill
Lives in the moment
|
The Real Calling
By Maria Sara Cueto, LECOM Seton Hill OMS-III
It took me years to realize,
but I eventually concluded
that my job
is not what I’d always pictured:
caring for others,
all smiles and all glory
with nothing left but satisfaction.
There is also grief. And loss. And worry.
|
No yes to the sweats
By Richard Donze, DO, MPH, PCOM '78
He only semi-tolerated the
semaglutide the nausea the
overfull feeling the belly bloat
but when his primary said they
could try others he realized he
disliked more the idea “like those
two sitcom friends one started
wearing sweatpants all the time
|
"I'm Listening:" A Nod to the 'Difficult' Patient
By Stephie Thomas, LECOM OMS-III
It’s hard to believe how quickly the third year of medical school has passed. One moment I was preparing for my first set of board exams and stepping nervously into rotations, and now I find myself studying for the next set of exams while reflecting on how much has changed. Watching my fourth year friends share their Match success stories feels different this year, more personal and real. In less than a year, I too will learn where I will spend the next stage of my training. That realization is both exciting and surreal.
|
My Not-So-Straightforward Path to Psychiatry
By D.R. Nanyes, DO, MBA, PGY-3, MSU/Pine Rest Christian Mental Health Services
I became interested in medicine soon after I joined the US Army. At my basic training graduation, my mother told me that she was recently diagnosed with cancer. The news was very difficult to handle, and I spent almost every day worrying if she would make it through the treatments. I would call home every chance I could get, as visits were hard to come by due to my service commitment and deployments. Each call home reminded me how uncertain the disease can be, and how harsh the chemotherapy side effects can be. I made it a goal that once my service was complete, I would do whatever I could to become a “cancer doctor” and find a better way to treat malignancies. As it was, I did not know anyone who went to college outside of my teachers back in high school, and I actually did not know “how” one becomes a doctor.
|
Rooted in Community:
A Student Reflection on Choosing Osteopathic Medicine for Rural Care
By Stephan Spolski, WVSOM OMS-I
As an EMT in my rural community, my eyes have been opened to the lack of healthcare for marginalized people. Schuylkill County is mainly comprised of low- to middle-income workers, and access to care is limited by the paucity of providers. It has been a shocking revelation that many people living in my own community are unable to receive appropriate medical treatment. Growing up in Schuylkill County, I’ve seen firsthand how limited access to healthcare can affect entire families and neighborhoods. Through conversations with local healthcare professionals and my own experiences in patient care, I have grown acutely aware of the urgent need for physicians who are dedicated to serving rural and underserved populations. This realization strengthens my resolve to become a well-rounded, compassionate physician who can address a broad range of health needs to serve any community.
|
With Appreciation, Thank You
By Ted Eisenberg, DO, PCOM '76
On Jan. 1, 1985, I began my practice as a plastic and reconstructive surgeon like many young physicians – with determination, optimism, and very few tangible assets. My wife was pregnant with our first child, and the responsibility to provide for my growing family was immediate and real. We made ends meet, though it was far from easy. I didn’t have an office of my own. What I did have was the extraordinary generosity of osteopathic colleagues. Five established PCOM physicians in the Philadelphia area – Drs. Laurence Belkoff, James Kantor, Daniel Wisely, Nicholas Pedano, and Dominic Bontempo, Sr. – opened their offices and shared their secretarial staff at no cost, telling me I could pay rent when I was able.
|
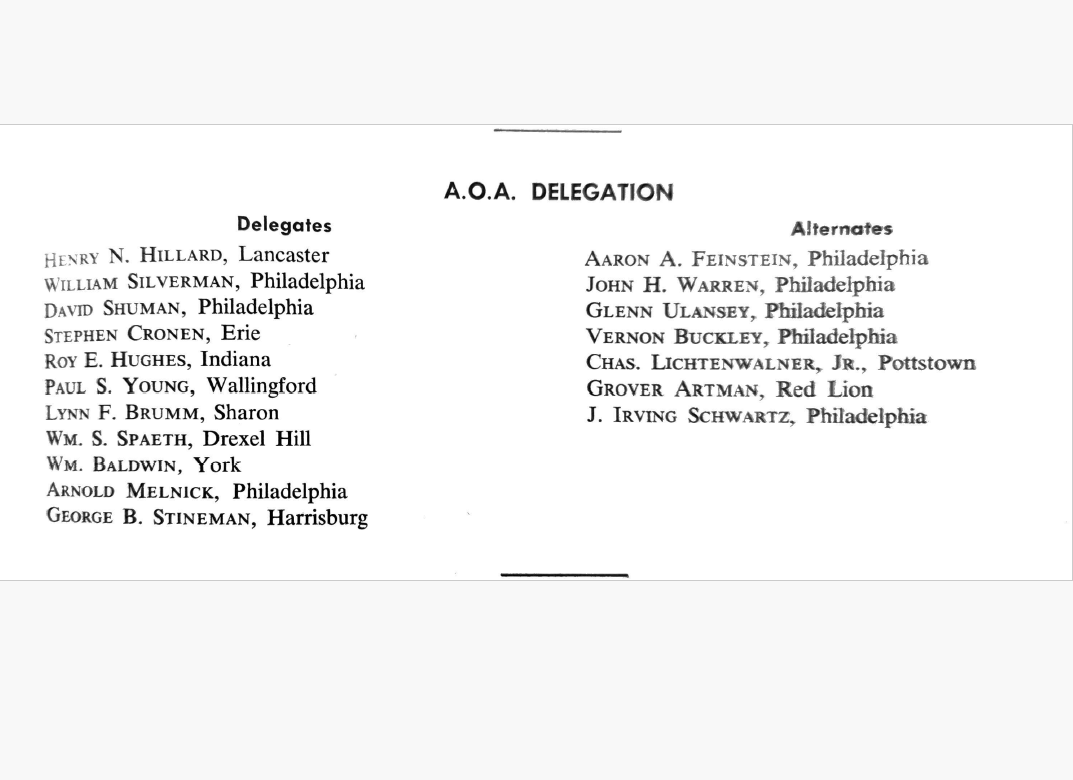
In just a few weeks from this publication, osteopathic physicians from across the country will meet in Chicago for the American Osteopathic Association’s annual House of Delegates meeting. This year, 43 delegates and 43 alternate delegates from Pennsylvania will attend, including four student delegates and four student alternate delegates. This page from the Winter 1961 issue of the Journal names the 11 delegates and 7 alternate delegates to the AOA. A lot has changed in the 65 years since these men attended the House of Delegates, but advocacy continues to be a driving force in osteopathic medicine.
|
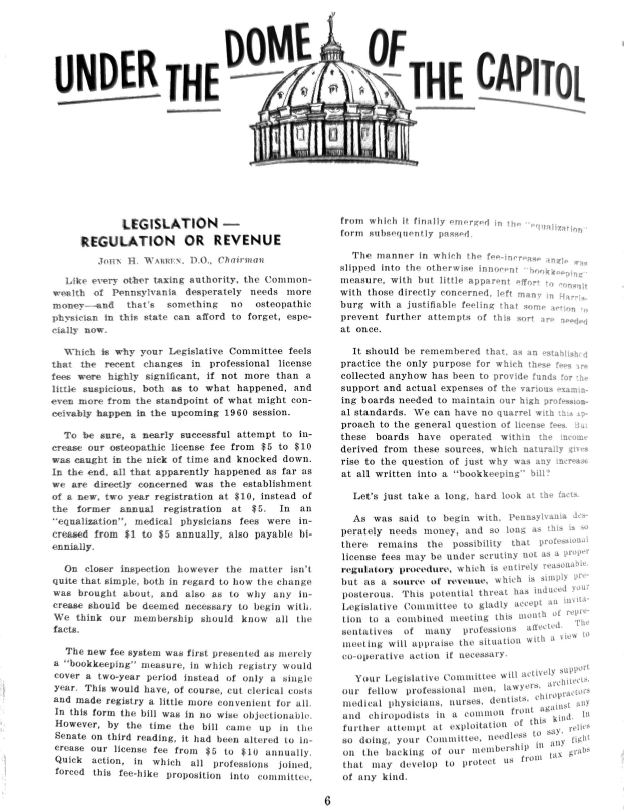
The Pennsylvania Osteopathic Medical Association, or the Pennsylvania Osteopathic Association as it used to be called, has always had a clear mission: to advocate for the osteopathic physicians in the state of Pennsylvania. Every month, POMA members receive an electronic issue of Under the Dome, updating all our members on the legislative moves over the past month. “Under the Dome of the Capitol” used to be published in the Journal, as it was in this Winter 1961 issue. This particular article highlighted the work that the legislative committee did to protest the increase in cost of an osteopathic medical license from $5 to $10 annually (ultimately, the cost remained at $5). It also highlights an effort by the state to treat allopathic physicians equally, as the cost of their medical license increased from $1 to $5 annually. While none of us now would protest a change in the cost of our medical license to $10, POMA’s government affairs committee meets monthly to review legislative changes and ensure our advocacy mission continues.
|
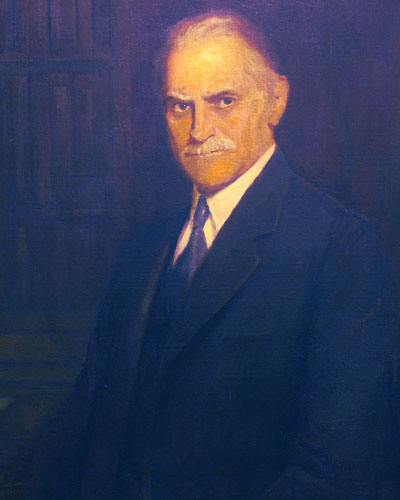
In honor of POMA celebrating its 103rd anniversary this month, the Guess Who is not only the founder of the Pennsylvania Osteopathic Association, as POMA was originally called, but he was also a co-founder of the Philadelphia College and Infirmary of Osteopathy and the first chair of the State Board of Osteopathic Medicine. He is truly a leader in osteopathic medicine in the state of Pennsylvania.
Click here if you can identify this founding leader osteopathic medicine in Pennsylvania!
The answer will be revealed in JPOMA's October 2026 issue.
(Answer to JPOMA's February 2026 Guess Who? - Nettie C. Turner, DO)
|
Members of our osteopathic community are the best and brightest. We honor the passing of these POMA members. We recognize their contributions and legacies to the profession and to POMA. To friends and families, we offer sympathies.
|
Publication Notes
Disclaimer
Views expressed in The Journal of the Pennsylvania Osteopathic Medical Association are solely those of the authors and do not necessarily reflect the opinions of the editorial board, The JPOMA, or POMA unless specified.
Letters to the Editor
We welcome your thoughts and feedback. Letters to the Editor may be submitted to [email protected].
About the JPOMA
Frequency
The Journal of the Pennsylvania Osteopathic Medical Association will be published three times a year: February, June, October.
Submission Information
The Journal of the Pennsylvania Osteopathic Medical Association is a safe space for all DOs to have a voice and be heard. Opportunities to contribute in all content areas are open to all osteopathic medical students, residents, and physicians. Share your thoughts, ideas, and submissions via email to [email protected].
Submission Deadlines
The Publications Committee will review submissions one month prior to publication. The rolling submission deadlines are as follows:
- January 15th for the February issue
- May 15th for the June issue
- September 15th for the October issue
Editorial Board
The POMA Publications Committee serves as the editorial board for the Journal of the Pennsylvania Osteopathic Medical Association. The committee is chaired by Joseph Zawisza, DO, and includes Richard Donze, DO; Katherine Galluzzi, DO; Samuel Garloff, DO; Porsche Lee, LECOM OMS-III; and Zachary Mendola, LECOM OMS-II. POMA President Angela Zawisza, DO, serves as champion of POMA's Communications Pillar.
|
|
|